
2017: Dr Gregor (retd): I Am A Unionist – Stages Career Comeback- Just For One day
Dr Gregor’s recent attack on the Scottish Health Service and Scottish Government was entirely expected.
A willing horse, she was trotted out by “Better Together” to deliver her poisoned views in the 2014 Independence Referendum.
At that time she said that she was not an avid “no” campaigner but she had issues with Alex Salmond who had claimed independence was needed to protect the Health service in Scotland from the Tory government in Westminster.
In her diatribe she also accused senior medical staff who supported Alex Salmond’s statement, of lying.
But her comments at the time she was interviewed on “www.radio.cz” and other publications, gives lie to he assertion that she was not an avid “no” supporter. She was and still is.
A brief review of events at the time she was Scotland Cancer Tzar (2001-2006) reveals a likely reason for her dislike of the SNP government.
In 2002 Dr Gregor brought forward a proposal to shut small local hospitals all over Scotland transferring healthcare finance to an American style operational mode.
Nicola Sturgeon (Shadow Minister of Health) and a number of senior Scottish Medical Officers supporting her opposed the measures and they were never carried through.
The American company has since been subject of much criticism over the years since. The then Labour Scottish Executive fortunate to have listened to Nicola Sturgeon’s counsel.
She is also memory blind to the poor state of the Scottish Health Service and cancer care services in the period 2001-2006.
The worst cancer services in Europe. Patients written off and dying often without any treatment or respite care.
Compare that record to the SNP government’s performance from 2007-2017. Cancer service provision in Scotland is rated one of the best in Europe.
And all this vitriol from an immigrant provided by the UK with free further education and extensive medical training and support leading to a rewarding career in cancer care.
And the galling fact that her own country, Czechoslovakia successfully split in 1993, reforming the Czech Republic and Slovkia in what has been termed: “The Velvet Revolution.” A well travelled road that Scotland would be wise to follow.
It might just be that not being native to Scotland Dr Gregor has failed to embrace the Dichotomy confronting Scots. But readers of the full article will be left wondering or just angry that she seeks to support the Westminster political system that so badly failed to protect it’s citizens.

Dr Anna Gregor Medical Consultant (Oncology)
Anna was born on 13 August 1948 in Prague, Czechoslovakia. She emigrated to England in 1970 to study and graduated from the Royal Free Hospital School of Medicine in 1973.
Her career path in medicine comprised: Senior house officer, registrar Brompton Hospital, Royal Marsden, London, 1973—1980. Consultant radiotherapist, oncologist Western Infirmary, Glasgow, Scotland, 1983—1987. Senior lecturer clinical oncology University Edinburgh, 1987—1997. Consultant clinical oncology, Macmillan lead cancer clinician Western General Hospital, 1997-2006.
Memberships: Fellow, Royal College Radiologists London, Royal College Physicians Edinburgh.
Anna’s time as a clinical oncologist in Edinburgh coincided with major changes in Scotland.
Following a transfer of political power in 1997, from the Conservative government to “New Labour” a referendum was held asking the Scottish electorate if it wished to take up devolved government.
The proposals received overwhelming support, with 74 per cent voting in favour of a Scottish Parliament and 63 per cent voting for the Parliament to have powers to vary the basic rate of income tax.
Following the passage of the Scotland Act 1998, the Scottish Executive (officially referred to as the Scottish Government since August 2007) and Scottish Parliament were officially convened in 1999, a date which marking the transfer of powers in devolved matters, previously exercised by the Secretary of State for Scotland and other UK Ministers, to the Scottish Ministers.
The Labour party were elected to form the first Scottish Executive.
The Scottish Health Service (SHS) was a devolved institution requiring the appointment of a Minister of Health and Susan Deacon was duly appointed.
She faced a baptism of fire in her new job as major deficiencies were identified across all services.
The National Health Service in Scotland, (controlled through the Scottish Office) had been badly neglected and starved of resources for years.
The organisation and delivery of cancer services was appalling. Survival rates were among the worst in Europe, in some areas the worst. Annually 26,000 Scots were being struck down with nearly 15,000 dying within 6 months.
It was so poor that in 1999 it overtook heart disease as the leading cause of premature death in Scotland. Susan Deacon had to act quickly and she duly did so.
She recruited Dr Anna Gregor to the cause, gave her a free hand and £40 million to fix things.
A strategy aimed at improving Scotland’s appalling record on cancer was duly unveiled by Susan Deacon.
Top Scots oncologist Dr Gregor was appointed to the new post of cancer supremo for Scotland.
As lead cancer clinician, she would head the strategy ensuring it delivered results on the ground.
There would also be a new approach to decision making and planning, bringing front line staff and patients together in a revamped Scottish cancer group giving them more say in deciding priorities for investment and change.
Three regional cancer advisory groups were created in the North, South-East and West of the country to improve the planning and design of local services, and to advise the Scottish cancer group on how to end the postcode lottery of care in Scotland.

The strategy also included:
1. Managed clinical networks, bringing together all professionals involved in caring for patients with a particular cancer type, to be in place by 2002.
2. All NHS boards to review local palliative care needs and services by March 2002.
3. Maximum waiting time from urgent referral to treatment for all cancers to be two months by 2005, with most patients treated faster.
Ms Deacon said the strategy’s aim was to build a comprehensive, modern network of services to match the best in Europe.
But this would be a long-term strategy – there was no quick fix to years of under-investment. She said: “Strong regional centres of excellence and regional cancer advisory groups will work with patients and the voluntary sector to make better local assessments of staff shortages and equipment needs. And our strengthened Scottish cancer group will ensure that money is directed where it is needed most,”
Dr Gregor, the new cancer supremo, said the group’s first priority would be to look at staff shortages in key specialities.
She would report to the minister by the autumn, with detailed plans before the end of the year. “This strategy marks a real watershed for cancer in Scotland. It offers us a real chance to start to speed up improvements in treatment.
But it is also a huge challenge for those of us delivering front line services. We have got to make the extra resources we have been given work better for patients,” she said.
The new strategy was welcomed as a “major step forward” by the British Medical Association in Scotland, which pledged to drive forward efforts to improve cancer care. “This is about more than just spending more, it also means putting clinicians in control and giving them the tools to improve every cancer patient’s chances of survival,” said Dr John Garner, chairman of the BMA’s Scottish council. (The Guardian)
Cancer Services in Scotland
What follows is a potted history of cancer care events in the period 2001-2008 at the time Dr Gregor had clinical management responsibility.

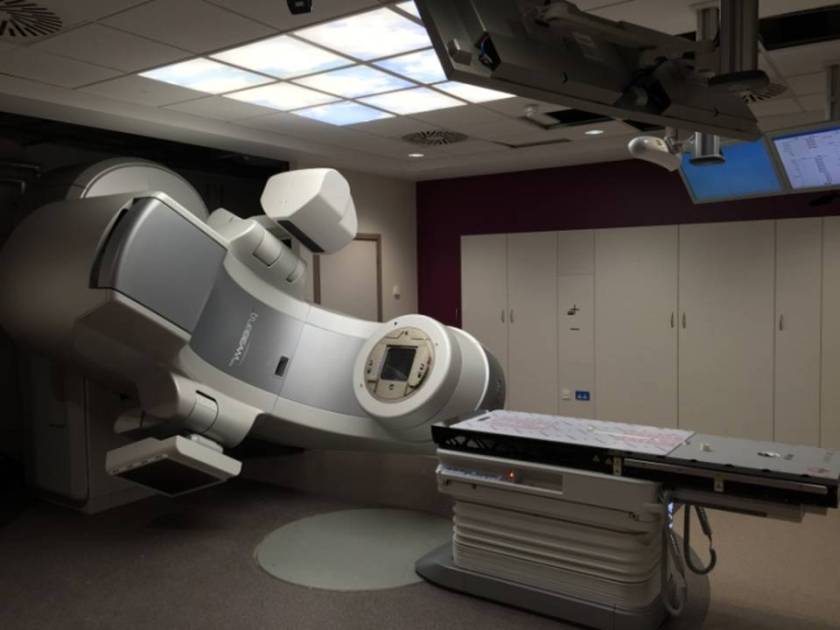
2001: Dr Gregor – Hospitals Need Twelve Linear Accelerators
Dr Gregor, oncology consultant and head of cancer services at Edinburgh’s Western General Hospital said: “the new equipment will ensure every cancer patient gets treated within the recommended four weeks” and estimated that it would cost only £18 million to buy and install it.
The cost represented just over half the £34 million which the executive had “clawed back” from the Scottish Health Service’s £135 million budget underspend.
comment: An underspend and the service in crisis. Unbelievable.
Additionally, each machine would cost about £200K annually to staff and run. She said: “We all know that there are unacceptable delays in the treatment of cancer, particularly lung cancer.” (The Herald)
2001: Cancer Expert: Why I Called Beatson a Slum
One of the world’s leading cancer experts has revealed he dropped his interest in a top job at Scotland’s main cancer centre after finding conditions at the hospital “like going into Bombay”.
Professor Karol Sikora was a candidate for the prestigious position of Chair of Oncology at the Beatson Centre in Glasgow but was put off by what he describes as “chronic under-investment”.
He was previously chief of the World Health Organisation cancer control programme and professor of clinical oncology at Hammersmith Hospital in London.
“I went to have a look. Half the patients in Scotland are treated there but the place is a mess.
It is one of the most prestigious positions in Scotland and arguably the biggest centre of its kind in Britain. (The Herald)
Comment: Some of the £135Million underspend should have gone to the Beatson

2001: Beatson Cancer Centre at “Breaking Point”
An urgent report has been demanded into the running of Scotland’s biggest cancer treatment centre after the resignation of three consultants and claims that the service is at breaking point.
Medical staff at the Beatson Oncology Centre in Glasgow, which treats 60% of all cancer cases in Scotland, have been concerned for some time that the rise in workload has not been matched by an increase in resources.
Although the Royal College of Radiologists recommends that consultant oncologists should only see 315 new patients a year, some of the oncologists at the Beatson are seeing twice that number.
The centre should have 11 linear accelerators to treat the population it serves, but it has only six.
The result is that waiting times are longer than recommended, and some doctors have warned that these delays are leading to poorer outcomes for some patients.
Professor of Radiation Oncology, Ann Barrett, is one of those leaving after 16 years at the Beatson centre. She blamed the lack of investment in the centre for her departure. “I am so unhappy that the quality of care I am able to give is so far below what I want that I simply find myself unable to carry on. Three of us leaving may well mean a crisis, but my hope is that by going I will help to push the issue forward so that something is done.”
The problems at the Beatson have led to difficulties in filling senior positions in the past. The post of professor of medical oncology has been vacant since 1999, and one applicant for the post, Professor Karol Sikora, abandoned his interest after publicly describing the Beatson as a slum.
Scotland’s health minister, Susan Deacon, asked for an urgent report on the problems at the centre.
Outside experts were called in to improve the management of the Beatson and to advise on the best way forward.
The row overshadowed an announcement the week before of extra resources for cancer care in Scotland.
Details were given of a £10m recruitment package that should increase the number of cancer specialists employed in Scotland, as well as extra nurses, radiographers, and other staff.
More than half of the money is to be spent in the area covered by the Beatson.
The investment is the first product of Scotland’s £40m national cancer plan that was launched in the summer.
Dr Gregor, the lead clinician in the Scottish Cancer Group, which identified the priority areas for action, said. “This is the first year of the cancer plan. Problems will not be solved overnight.
But we have a responsibility to make sure that this investment makes a real difference.” (http://pubmedcentralcanada.ca/ptpicrender.fcgi?aid=327273&blobtype=html&lang=en-ca)

2001: Dr Gregor and Her £40 Million Blueprint For Reforming Cancer Care in Scotland
A champion of patient involvement in health care planning and policy, she said, that she wanted to seize the “historic opportunity” to change cancer care in Scotland for the better dismantling “many fundamental barriers to change in the NHS”. (The Herald)

2001: Radical changes in fight on cancer; New strategy bids to overcome failings
The Scottish cancer strategy promises a radical new approach to a disease which strikes and kills many thousands of Scots each year.
The plan acknowledges failings in the past lack of investment in modern equipment, poor workforce planning to meet demand and badly organised services to treat patients quickly and sensitively.
Three new groups will be created to improve planning and design of local services to end the postcode lottery of care when access to services is determined by where the patient lives. (The Herald)

2001: Management and survival of Patients With Lung Cancer in Scotland Diagnosed in 1995: Results of a National Population Based Study.(Report compiled by Dr Gregor)
Background: The prognosis of patients with lung cancer in Scotland is poor and not improving. This study was designed to document factors influencing referral, diagnostic evaluation, treatment, and survival in patients with lung cancer.
Methods: Patients diagnosed during 1995 were identified from the Scottish Cancer Registry and their medical records were reviewed. Adequate records were available in 91.2% of all potentially eligible cases.
Results: In 1995, 74.1% of patients in Scotland diagnosed with lung cancer had the condition confirmed through laboratory testing. And 75.3% were assessed by a respiratory physician;
However, only 56.8% received active treatment (resection 10.7%, radiotherapy 35.8%, chemotherapy 16.1%) and 2.9% participated in a clinical trial.
Survival was poor with a median of 3.6 months; 21.1% were alive at 1 year and 7.0% survived 3 years.
Conclusion: This national population based study demonstrates low use of treatment, poor survival, and the influence of process of care on survival. Implementation of evidence-based guidelines will require substantial changes in practice. Increasing the number of patients who receive treatment may improve survival. (https://www.ncbi.nlm.nih.gov/pubmed/11182014)
2001: Cancer Scenarios: An Aid to Planning Cancer Services in Scotland in the Next Decade
The population of Scotland experiences relatively high incidence of many common cancers, and deaths from cancer represent a significant fraction of total mortality.
Within Scotland, there are significant variations in the risk and outcome of cancer, geographically and socially.
This grim picture is moderated to some extent by the knowledge that we have the tools at hand to do something about it in a rational way.
Collection of reliable data on cancer incidence and outcome, and health professionals committed to use of information to improve services through evidence-based practice.
The aims of the Scenarios project are to predict trends in cancer incidence and mortality in Scotland in the next decade, and to speculate on the scope to influence these trends through interventions such as screening programmes and the application of recent innovations in treatment.
The purpose of the report is to bring together this information as an aid for the planning of cancer services in the next decade. (http://www.sehd.scot.nhs.uk/publications/csatp/csatp-00.htm)
2001: Scandal of the Cancer Patients Left to Die-Calls for Inquiry Into Ageism in NHS
Around 800 Scots a year diagnosed with lung cancer do not get the treatment they need, according to a new study.
The same report revealed that only 31% of patients older than 70 were treated, a finding which last night prompted charities for the elderly to call for an investigation into ageism in the health service.
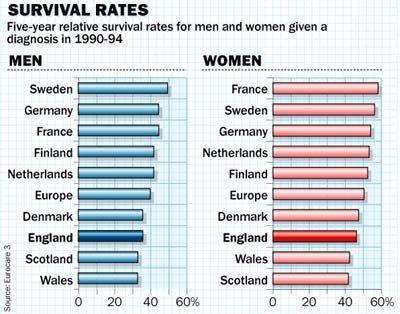
Scotland has the worst record in Europe for a disease which strikes without mercy.
Fewer than 5% of patients survive after five years compared to 14% in other European countries.
The Scottish survival rate has changed little in 25 years, despite new treatments.
A rise in deaths in the early 1990s alongside a drop in numbers diagnosed showed deficiencies in treatment. (The Herald)

2002: Dr Gregor – Warns That Planned Improvements Are in Jeopardy Due To a Shortage of Trained Staff
Cancer services in Scotland have been subject to sustained bad publicity in the media for the last year.
Against a background of low five-year survival rates for lung cancer compared to the rest of the UK and Europe, for example, specific services have been widely criticised.
A recent Cancer Research UK survey found that some surgeons in Scotland have been failing to follow guidelines on staging endome-trial cancer.
The report, published in the British Journal of Cancer, concluded that death rates were ‘significantly higher’ where guidelines were not followed although other factors would also influence patient outcomes.
Dr Anna Gregor, a leading cancer clinician for Scotland, warned that the Scottish Executive’s plan to improve cancer care is being hindered by a lack of expert staff. (http://journals.rcni.com/doi/pdfplus/10.7748/cnp.1.6.9.s14)
2002: Dr Gregor Warns of delay to NHS cure
Dr Anna Gregor, lead clinician for cancer services in Scotland, warned that the fight against the disease was about more than resources and said getting the right numbers of trained staff in place could take years.
Speaking at the Scotland Against Cancer conference, hosted in Edinburgh by the Scottish Parliament’s cross-party group on cancer, she said: “If I got £100 million to spend on staff today I couldn’t get them.
There is a severe shortage of trained manpower, of oncologists, radiographers, radiologists. I’m told we’ve run out of cancer nurses and specialist cancer pharmacists.” (The Herald)

2002: Dr Gregor – Scotland’s Cancer Czar Tells Health Secretary to Shut Little Hospitals and Spend The Money Saved On American Style Rapid Outpatient Care.
The Labour government appointed cancer expert said “We can do with fewer hospitals, absolutely.
Every time you try and close one somewhere the politicians march out, local clinical groups march out and patient groups march out”. But better results would be achieved by concentrating resources on modern equipment, more specialist clinicians and shorter stays for patients.
But her comments went against the conventional wisdom that more beds are needed to speed up the treatment of patients, thousands of whom are facing long waits for operations in Scotland.
But The Scottish Executive backed her remarks, which came just weeks after she and health minister, Malcolm Chisholm made a fact-finding visit to the United States.
She said she had been impressed by the care system used by Kaiser Permanente, an American private healthcare provider.
She said: “Patients face shorter waits and have access to a larger number of specialists and more modern equipment, partly as a result of money being saved by using fewer costly hospital beds and having shorter inpatient stays.
Kaiser Permanente’s use of hospital beds is a third of that of the NHS and Scotland has more beds than the rest of the UK.
It’s absolutely the way we should go. We need to have a radical rethink, stop emptying people into beds because we have such long waiting times. It clogs up the system and costs money.”
Shadow health spokeswoman Nicola Sturgeon opposed the suggestion that the number of hospital beds in Scotland should be cut.
She said: “It’s completely the wrong thing to do. We have 700 fewer acute beds now than we had in 1999 and it is one of the reasons we have struggled to get waiting lists and waiting times down.”
Report available: (http://www.kaiserthrive.org/kaiser-permanente-horror-stories/)
The Scottish organiser for Unison, said Kaiser Permanente had faced heavy opposition from health unions in its home state of California.
He said: “They launched a campaign under the heading of: ‘Sicker and Quicker’. By making primary care the priority and reducing the number of acute beds Kaiser Permanente patients are being admitted sicker and are being discharged quicker.”
Dr Harry Burns, Director of Public Health at Greater Glasgow Health Board, also said he was not convinced by the American model. He warned the study published in the BMJ was “deeply flawed” because it did not take higher social deprivation in Britain fully into account.
He said: “With Kaiser you have your cardiac surgery at Stamford University and then go back to a million-dollar house in Palo Alto.
If you have your cardiac surgery in Glasgow you go back to a fourth-floor tenement flat in Shettleston.”
Dr John Garner, chairman of the British Medical Association in Scotland, also warned against further reductions in the number of beds, explaining a large proportion were needed for emergency admissions.
And Margaret Davidson, of the Scotland Patients’ Association, condemned Gregor’s suggestion that some local hospitals should be allowed to close.
The Scottish Executive said it welcomed Gregor’s comments and shared some of her views.
A spokesman said: “Bed numbers should not be the currency on which we judge the success of the NHS.
What is far more important is to look at the patient and how their journey of care through the system is managed.”
(http://www.scotsman.com/news/cancer-czar-shut-down-hospitals-to-fund-care-1-1373489)
2002: Lack of Specialised Staff Putting Dr Gregor’s Scotland’s Cancer Plans at Risk of Failing
Dr Anna Gregor, leading cancer clinician for Scotland, told a conference in Edinburgh that the health service was “running out” of vital staff. “The biggest difficulty is the current shortage of trained manpower,”
Dr Gregor revealed. “We are running out of trained cancer nurses and we have run out of trained oncology pharmacists. We need a national strategy to address this,”
Dr Gregor’s comments came two months after Malcolm Chisholm, the health minister, announced an extra GBP 10 million for cancer services, some of which was to be spent on recruiting more nurses. (The Scotsman)
2003: Dr Gregor – The Doctor Who Has Seen How the System is Failing Cancer Patients
Dr Gregor explained why she had undertaken the thankless task of overhauling the delivery of cancer services for Scotland. “I decided that the last ten years of my working life would be spent trying to fix the system,” she says, the clipped vowels of her native Prague still faintly audible. “I had grown really tired of trying to fix things for individual patients. It was becoming increasing difficult. However much I improved the bit I was responsible for, the die was cast by the time the patient got to me and I could not influence what would happen to them after they left my care. Things needed to be changed. (The Scotsman)
2003: Dr Gregor Highlights Scotland’s Cancer Timebomb
According to Dr Gregor, lead clinician for cancer services in Scotland, the incidence of cancer in Scotland is set to rise by between 20 and 40 per cent in the next ten years.
Currently, 26,000 Scots are diagnosed with cancer each year and 15,000 die of it.
By 2013, the figure for those contracting cancer could be as high as 36,400 but death rates are set to fall, increasing the pressure on an already over-stretched NHS. (The Scotsman)

2004: Dr Gregor Warns of Crisis in NHS Services Unless Urgent Action is Taken
Dr Gregor, the lead cancer clinician for Scotland and the woman whose job it is to implement the Scottish Cancer Plan, said Scotland lacks an overall vision for the future of NHS services.
She is calling for a wide-ranging public debate about the future direction of the NHS in Scotland. “Whether it is an ideological barrier or a political one I don’t know, but there is an unwillingness to do the difficult things that need to be done,” she said.
She went on to state that: “the NHS in Scotland has been cushioned from the sort of pressures the NHS in England is currently facing because of the extra 20 per cent funding it has traditionally received under the Barnett formula. (The Scotsman)

2005: Dr Gregor Calls For a Tax On the Big Mac and Other Fast Food To Help in the Fight Against Cancer
Dr Gregor said a tax on McDonald’s burgers could cut the amount of fatty foods consumed, just as high duty on cigarettes had cut smoking rates.
Appointed by the Scottish Executive to oversee reform of Scotland’s cancer services, she believes a poor diet and reliance on junk food is at the heart of the country’s poor health record.
And she wants any revenue brought in from the new tax to be reinvested in healthy eating programmes. ‘If we are serious as a country about changing the population’s eating habits, then we have to look at the tools at our disposal, including pricing policy,’ Dr Gregor said. ((The Scotsman)

2006-2008 Dr Gregor was awarded CBE for services to Medicine. She retired in 2008 and took up work with “Prostate Scotland” which had been set up in 2006 as a registered Scottish charity to inform, support and advance on prostate disease and prostate cancer.

2014: Scottish Expats in Prague Frustrated to be Missing Out on Independence Vote
Unlike Scottish ex-pats, thousands of EU nationals living in Scotland are entitled to take part in the vote.
That includes an estimated 7,000 Czechs some of whom are temporary labourers while others are long-terms residents. One of the latter is Doctor Anna Gregor, CBE.
She left Czechoslovakia for Britain in 1969, and eventually settled in Edinburgh, becoming one of Scotland’s leading oncologists. She is opposed to Scotland’s independence.
She is also unhappy that temporary residents have a say. “We had an invasion of Catalans to Scotland who have an interest in the vote because of their own separatist agenda. A crass observation
We’ve had Poles – but they eventually realize that if they vote yes and we as a secession state will cease to be in the EU until we manage somehow to get back, they will have to leave. ” Another crass observation

2014: Lies, Damn Lies, and Statistics – Dr Gregor (Retd)
Formerly a leading cancer clinician in Scotland, Dr Gregor (retd), attacked the “Yes” campaign assertion that Scotland needed to gain independence to protect the Scottish NHS.
She stated that this was a “total and utter lie” and went on to express her concern about the “unreasonable distress and panic” that was being spread among patients.
But the “Yes” campaign had its own selection of health experts, and the campaign group NHS for “Yes” boasted a growing list of members, including Professor Mike Lean from Glasgow University and consultant surgeon Phillipa Whitford, who support their belief that the best way to protect the NHS in Scotland was through independence.
Scotland’s esteemed former chief medical officer, Sir Harry Burns, also argued that Scottish independence could be “very positive” for the country’s health, if people felt they had more control over their lives.
It is clear that by attempting to shift the focus to the health service the SNP has managed to strike a nerve amongst their opponents, but whether it strikes a chord with the public remains to be seen. (Holyrood)

2017: Dr Gregor (Retd 2014) Claims NHS On Cliff Edge As SNP Starves Services of Cash,
The now retired doctor, (who has repeatedly criticised the SNP government for their handling of the devolved NHS since coming to power in 2007) blasted the Scottish Government for not passing on cash increases from Westminster to cancer care.
Dr Gregor once credited with leading Scotland’s cancer care strategy from near disaster (under Labour and LibDem Executives) to recovery, said that Nicola Sturgeon’s party have failed to meet a series of waiting time and treatment targets.
She went on: “We are hurtling over a precipice with everyone pretending that it is going to be all right and it won’t be.
If you have a health service tightly controlled by politicians, then you have additional complexities in this already messy system, which is short-termism and pork-barrel politics of the highest order.
She added: “Until about 10 years ago, we could have put the NHS on a sustainable footing.
Ten years ago we didn’t have a 25 per cent vacancy rate in senior clinical staff. “We didn’t have budget shortfalls.
We didn’t have such demoralised staff that they were all looking to protect their pension pots and going at 55. “We can’t get people to come here.
The politicians are being extremely disingenuous when they say we want a health service fit for the 21st century. “They are doing nothing to make that happen. Quite the opposite, they are stopping things from happening.”
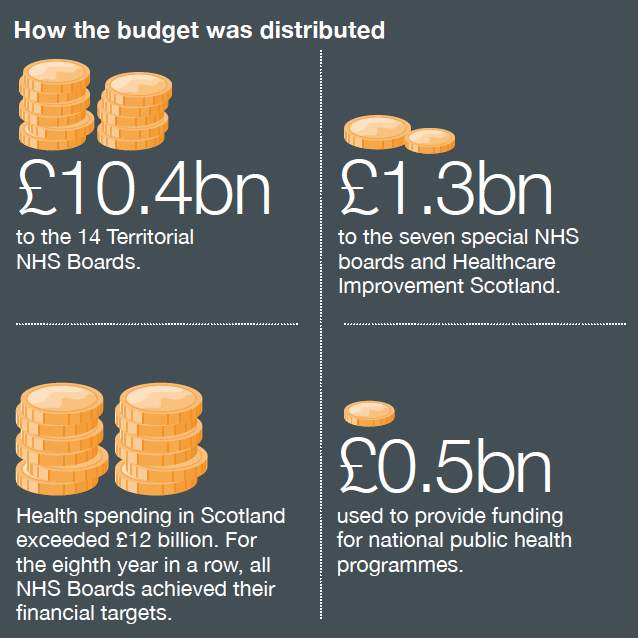
The NHS spend £12.2 billion a year in Scotland, about 40 per cent of the total Scottish budget.
But Treasury figures show a nine per cent increase in health spending in England, compared with a 3.4 per cent rise in Scotland between 2011-16.
NHS boards have been asked to make savings of £500 million an average of 4.8 per cent, this year. All of which will be reinvested in the Service which will assist matters.
The Scottish Government insisted they are committing an additional £327 million to health boards, taking NHS funding to a record high level and delivering £176 million more than inflation.
A spokesman said: “This reflects our commitment to protect the NHS with record levels of investment and is an important step towards achieving our commitment to increase the front line NHS budget by almost £2 billion by the end of this parliament.” (Daily Record)

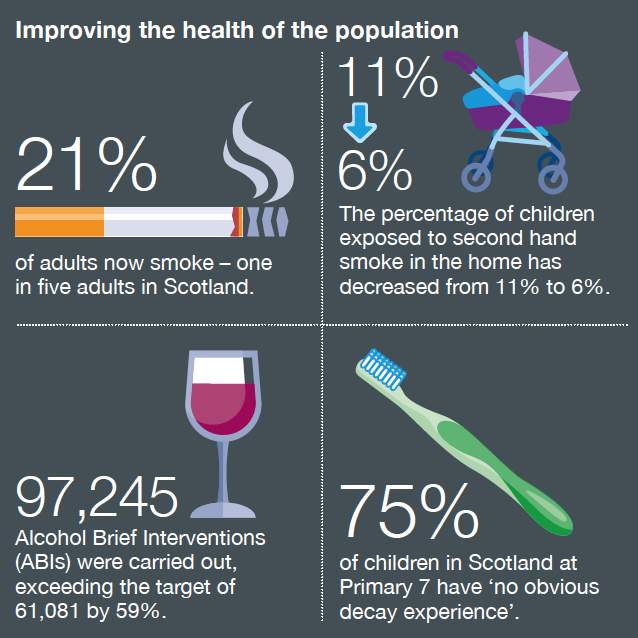
6 May 2017: But her claims do not match the facts – Health Service Patient Satisfaction Continues to rise in Scotland
Health Service Provision in Scotland Can be likened to “James and the Giant Peach” It’ll Swallow Up all the Available Resources and Still Want More
2017: We spend 35% of Scotland’s budget on health and this year we will spend more than £12bn on the health of 5.34m souls.
According to Dr Anna Gregor, formerly the lead cancer clinician for Scotland, health statisticians have worked out that if we carry on with the same healthcare provision as we have now, the increasing demand will mean that by 2025, every school leaver in Scotland will be required to work for the NHS.
(Here she is indicating a review of health service provision is needed cutting back reducing staffing requirements)

2017 Summary:
Dr Gregor’s recent attack on the Scottish Health Service and Scottish Government was entirely expected.
A willing horse, she was trotted out by “Better Together” to deliver her poisoned views in the 2014 Independence Referendum.
At that time she said that she was not an avid “no” campaigner but she had issues with Alex Salmond who had claimed independence was needed to protect the Health service in Scotland from the Tory government in Westminster.
In her diatribe she also accused senior medical staff who supported Alex Salmond’s statement, of lying.
But her comments at the time she was interviewed on “www.radio.cz” and other publications, gives lie to he assertion that she was not an avid “no” supporter. She was and still is.
A brief review of events at the time she was Scotland Cancer Tzar (2001-2006) reveals a likely reason for her dislike of the SNP government.
In 2002 Dr Gregor brought forward a proposal to shut small local hospitals all over Scotland transferring healthcare finance to an American style operational mode.
Nicola Sturgeon (Shadow Minister of Health) and a number of senior Scottish Medical Officers supporting her opposed the measures and they were never carried through.
The American company has since been subject of much criticism over the years since. The then Labour Scottish Executive fortunate to have listened to Nicola Sturgeon’s counsel.
She is also memory blind to the poor state of the Scottish Health Service and cancer care services in the period 2001-2006.
The worst cancer services in Europe. Patients written off and dying often without any treatment or respite care.
Compare that record to the SNP government’s performance from 2007-2017. Cancer service provision in Scotland is rated one of the best in Europe.

